How FHIR is Redefining Healthcare App Development: Interoperability, Compliance, and ROI

Table of Content
- Why Proprietary Healthcare Integrations Are Failing at Scale?
- What Is FHIR and How Does It Actually Work in Healthcare App Development?
- 7 High-Impact FHIR Healthcare App Development Use Cases
- FHIR-Based Development vs. Proprietary Integration: The Real Cost Comparison
- FHIR Implementation Timeline: A Phased Roadmap for Healthcare App
- Why the Right Implementation Partner Cuts Your Timeline From 24 Weeks to 14?
- How MultiQoS Compresses This to 14 Weeks?
- Conclusion
- FAQs
Summary :
This guide breaks down why proprietary EHR integrations are failing, vendor lock-in, compliance liability, maintenance cost spiral, and innovation bottleneck, and explains how FHIR R4 + SMART on FHIR actually works as an operational architecture. Covers 7 high-impact use cases from patient portals to AI clinical decision support, a real cost comparison between FHIR-based and proprietary point-to-point integration, and a 4-phase, 20-week implementation roadmap from discovery to production rollout. Built for health tech teams evaluating their next EHR architecture decision.
73% of digital health companies now rely on FHIR APIs for EHR integration. That number is not a trend. It is a compliance trajectory. The 21st Century Cures Act already mandates FHIR-based patient data access, and the proposed HTI-5 rule would eliminate more than 50% of legacy certification criteria in favor of FHIR API integration.
FHIR healthcare app development, built on REST APIs, JSON, and OAuth 2.0, enables real-time, secure clinical data exchange across any EHR system without rip-and-replace migrations.
This guide covers the real cost comparison, a phase-by-phase implementation roadmap, seven high-impact use cases, and the compliance framework your team needs before the next architecture decision.
Why Proprietary Healthcare Integrations Are Failing at Scale?
Most healthcare organizations did not choose proprietary integrations. They inherited them. Four failure modes are now compounding that decision.

Vendor Lock-In and Healthcare Data Silos.
Proprietary EHR integration solutions bind your organization to a single vendor’s update cycle. Every new system connection requires a custom build from scratch: no portability, no reuse. The result is a healthcare data silo that blocks every downstream initiative, from patient portal FHIR API development to real-time clinical data exchange.
Compliance Liability.
The proposed HTI-5 rule would remove more than 50% of legacy certification criteria. Organizations running proprietary stacks are not just accumulating technical debt. They are building regulatory exposure that compounds with every enforcement cycle. FHIR-based EHR modernization is no longer a roadmap item. It is a compliance deadline.
Maintenance Cost Spiral.
Custom point-to-point EHR integration solutions consume 20 to 30% of their original development cost every year in ongoing maintenance. According to Gartner, 83% of data migration projects fail or exceed budget thresholds. Healthcare migrations carry additional patient safety stakes. Every broken interface is a potential care coordination failure.
Innovation Bottleneck.
Legacy integrations cannot support healthcare AI FHIR data pipelines, wearable device EHR data exchange, or real-time clinical analytics. SMART on FHIR app development enables app portability across Epic, Cerner, and other EHR platforms without rebuilding from scratch. Organizations still on proprietary stacks cannot access that speed.
What Is FHIR and How Does It Actually Work in Healthcare App Development?
FHIR stands for Fast Healthcare Interoperability Resources and is an operational architecture for healthcare software development. It is developed by HL7 (Health Level Seven International) for healthcare organizations for the exchange of data electronically.
Take an example of the electronic health record (EHR) system of a hospital. Often, EHR systems don’t have the capability to share data with a local clinic’s system, and even a patient’s personal health app built in. This is where FHIR API integration helps. It standardizes the data exchange across systems, ensuring seamless patient care and health monitoring.
FHIR is basically a set of rules that acts as a universal language for digital healthcare systems. Conventional healthcare systems use outdated approaches like sending messages back and forth to exchange data. FHIR uses modern internet technology to power data exchange much faster and securely across all digital healthcare systems.
The difference between conventional systems and FHIR-based systems is how data is sent across platforms. Instead of sending massive files containing the entire medical history of a patient, FHIR breaks down information into modular categories.
For example, if it’s patient profile data, FHIR categorizes it as the “Patient Info.” Similarly, there is one for medications and another for symptom tracking data.
What is “SMART on FHIR”?
SMART on FHIR is like Google login on any app. It allows a health app to securely prove its identity and connect to major hospital software systems. This works without developers needing to build a custom and complicated login system.
7 High-Impact FHIR Healthcare App Development Use Cases
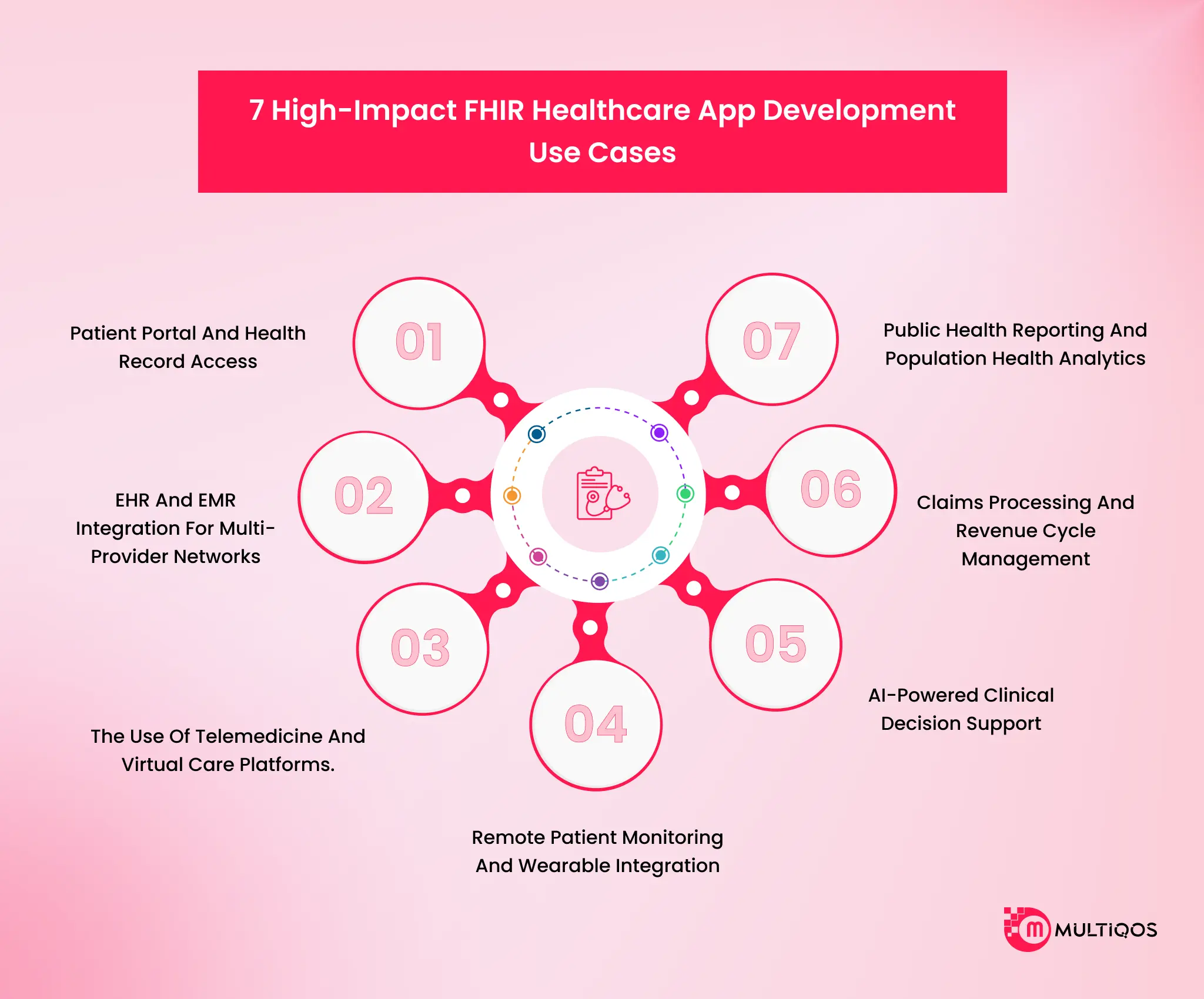
Patient Portal and Health Record Access
The problem is fragmentation. A patient with three treating providers has three separate records, three separate portals, and no unified view of their own health history. FHIR Patient and DocumentReference resources solve this by enabling standardized read access across participating systems.
70% of hospitals now allow patient access via FHIR apps, according to ONC data. The operational outcome is measurable: reduced call volume to medical records departments, lower administrative overhead for record release requests, and higher patient engagement scores that directly affect value-based care reimbursement.
For health tech teams, this is one of the fastest FHIR use cases to ship patient demographics, and document retrieval is among the simplest FHIR resources to implement and the highest-visibility outcomes to demonstrate to hospital system clients.
EHR and EMR Integration for Multi-Provider Networks
The problem is integration timelines that kill product velocity. A health tech company building a care coordination platform that needs to integrate with Epic, Cerner, and Meditech using proprietary interfaces is looking at 6 to 18 months of engineering time, per vendor.
FHIR R4 standardizes that work. Bidirectional sync across major EHRs using SMART on FHIR authentication compresses that timeline.
The business impact for a Series A digital health company is significant: faster time to market, lower burn rate on integration engineering, and a product architecture that scales to new EHR partners without starting from scratch.
MultiQoS has been responsible for multi-EHR FHIR integration projects, which have spanned the entire lifecycle from discovery to production sync in less than 14 weeks, for healthcare clients.
The use of Telemedicine and Virtual Care Platforms.
Documentation gaps are the issue. With virtual visits comes clinical data, vital signs, chief complaints, and encounter notes; these should be transferred back to the patient’s EHR for continuity of care. That data transfer is manual, delayed, or lost if it doesn’t happen with FHIR integration.
The FHIR Observation resources are the standard way to pass biometric data and clinical data from a virtual care platform directly to the EHR, and in real time.
This takes away one type of clinical risk from telemedicine platforms and one of the most common issues on the care team’s list: They can’t see what happened in the virtual visit. The downstream effect of the lower burden of documentation by clinicians and better-informed follow-up care.
Remote Patient Monitoring and Wearable Integration
The primary challenge with remote monitoring is getting actionable data to the clinician. A continuous glucose monitor can generate thousands of readings a week, but without FHIR, that data sits isolated in a vendor’s cloud.
With FHIR, that information is in a vendor’s cloud, separate from the EHR, and inaccessible to health care staff. Observation resources provide a capability for every clinical measurement, including blood pressure, glucose, activity, oxygen saturation, and more, to be measured in a clinically meaningful manner, allowing for IoT and wearable devices to send data directly to FHIR endpoints.
This provides a closed-loop monitoring system, and clinicians are able to view device data and lab results, medication lists, and encounter notes all within a single clinical record. It’s the backbone technology that healthcare application development teams must have to construct reliable remote monitoring programs.
AI-Powered Clinical Decision Support
AI models require clean and structured, standardized clinical data. Without FHIR, the requirements for building an AI/ML pipeline for clinical decision support are custom ETL work for each data source, each EHR vendor, and each site.
Utilizing the native FHIR R4 stores in Google Healthcare API, users can connect directly to BigQuery and Vertex AI, allowing for ML pipelines to run on standard clinical data without any custom extraction logic.
FHIR is the data infrastructure layer that enables AI in healthcare compliance and model deployment in an 18-month timeframe, not in isolation but in combination with model building.
Predicting readmission risk is a prime example of how FHIR accelerates AI in healthcare compliance, an deployment turning an 18-month infrastructure nightmare into a streamlined process.
Claims Processing and Revenue Cycle Management
The problem is manual claims routing and high denial rates driven by missing or misformatted data. FHIR ExplanationOfBenefit and Claim resources define standardized data structures for claims submission, adjudication, and remittance.
Payers and clearinghouses building on FHIR R4 can automate claims routing based on structured data rather than paper-equivalent EDI transactions. The operational impact is a 60% improvement in underwriting turnaround for organizations that have migrated from proprietary claims interfaces to FHIR-native workflows.
For revenue cycle management platforms, FHIR also enables real-time eligibility verification and prior authorization automation using the CDS Hooks framework.
Public Health Reporting and Population Health Analytics
The problem is that public health agencies cannot act on data they cannot receive. Fragmented reporting systems mean disease surveillance data is delayed, incomplete, and incompatible across jurisdictions.
FHIR enables standardized data submission to state health agencies and CDC infrastructure through the Electronic Case Reporting (eCR) framework.
For population health platforms, FHIR Group and MeasureReport resources enable standardized quality measure calculation and reporting across attributed patient populations, the data infrastructure behind value-based care program performance.
CMS quality reporting programs are moving to FHIR-based data submission requirements with enforcement timelines already set.

FHIR-Based Development vs. Proprietary Integration: The Real Cost Comparison
The cost difference between FHIR-based development and proprietary point-to-point integration is not marginal. It is structural. Proprietary integrations frontload engineering cost and then sustain it indefinitely. FHIR-based architecture distributes costs more efficiently across a larger connected surface.
| Comparison Dimension | FHIR-Based Development | Proprietary Point-to-Point Integration |
| Initial development cost | $40,000–$120,000 for core FHIR implementation with SMART on FHIR auth | $80,000–$250,000+ per EHR vendor, custom per interface |
| Integration timeline | 6–12 weeks for first EHR connection | 6–18 months per EHR vendor |
| Per the additional EHR vendor | Incremental configuration, minimal rework (SMART on FHIR portability) | Full custom build per vendor, $80K–$200K+ each |
| Annual maintenance burden | 8–12% of initial development cost (standards-based, stable API contracts) | 20–30% of initial cost annually (brittle custom interfaces, EHR version dependency) |
| Compliance overhead | FHIR built-in AuditEvent, TLS 1.2+, OAuth 2.0 — compliance-ready by default | Custom audit logging, custom encryption, per-vendor compliance review |
| Scalability | Add new EHR partners, data types, and use cases on the existing foundation | Each new connection = new project, new budget, new timeline |
| Long-term cost trajectory | Decreasing marginal cost per additional integration | Flat or increasing — no economies of scale |
| Regulatory risk | Aligned with the 21st Century Cures Act, ONC mandates, HTI-5 trajectory | Exposed to enforcement risk as legacy certification criteria phase out |
The break-even point typically occurs at the second or third EHR integration. A healthcare platform connecting to five EHR systems on proprietary interfaces is spending $400,000 to $1,000,000 in integration engineering alone before accounting for annual maintenance.
For teams building on custom software development infrastructure, the FHIR cost advantage compounds over time. Proprietary integrations do not get cheaper. FHIR-based architectures do.

FHIR Implementation Timeline: A Phased Roadmap for Healthcare App
The biggest pitfall of implementing FHIR is attempting to develop it all at once. On day one, organizations that try to force a complete bidirectional sync of all data types routinely end up in pilot purgatory projects that never get to production.
The right approach is incremental, delivering usable features into production at the end of each phase.
Phase 1: Discovery and Planning (Weeks 1–3)
Identify the specific FHIR use cases that you’re going to be supporting in your initial deployment. Avoid spreading out the scope of work in this stage. Review your current systems to determine their data quality, API readiness, and EHR vendor FHIR level.
Before starting the architecture, one needs to determine which resources of the FHIR library will be exposed by a particular EHR instance, as not all of them will be exposed.
Have the appropriate team: Product Owner with clinical workflow knowledge, FHIR Specialist, Cloud DevOps engineer, and QA with healthcare domain knowledge.
Outline compliance requirements, HIPAA technical safeguards, BAA structure for interoperability circumstances, and state-level data residency requirements.
Phase 2: Architecture and Data Modeling (Weeks 4–6)
Map your data model to FHIR resources. Create SMART on FHIR authorization flow scope, launch context, and open lifecycle management.
Make the API Gateway layer an interlayer between your app and EHR FHIR endpoints. Implement technical security controls compliant with HIPAA: AES-256 encryption at rest, TLS 1.2+ encryption in transit, and audit logging with FHIR AuditEvent resources.
Outline the conformance profiles that your implementation will conform to. This is where you define the FHIR that you will use for your use case in a formal way, and QA can then have a testable specification.
Phase 3: Build, Test, and Validate (Weeks 7–14)
Development for the API based on the architecture designed in Phase 2. Conformance testing of FHIR resources in scope. There are several different types of integration testing that can be performed, with each approach having its own advantages and disadvantages.
There are three main forms of integration testing: integration against target EHR sandbox environments, Epic, Cerner, and Meditech, with each providing access for EHR development and testing purposes.
Performance hardening: Do your tests with a realistic patient volume while running concurrent API calls and make sure that your response times are within your clinical workflow. Mobile app development teams that are to create HIPAA-compliant mobile apps should view this stage as the compliance check prior to any production of patient data under the system.
Phase 4: Pilot Deployment and Production Rollout (Weeks 15–20)
Implement a canary deployment pattern to deploy to a single clinical site, route a controlled %age of real patient data through the FHIR integration, and have a fallback to the legacy system.
Set up monitoring: Response time of FHIR API, Error rate by resource type, Rate of failure to authenticate, AuditEvent logs completeness. Get feedback from clinical end users in structured feedback loops. Their workflow friction during the pilot is your most valuable sign of production optimization.
Successful pilots result in full production rollout, and a governance process that sets the principles and oversight of who will be making schema decisions for FHIR, principles of versioning an API, and principles of managing relations with EHR vendors.
Why the Right Implementation Partner Cuts Your Timeline From 24 Weeks to 14?
The 4-phase roadmap above is accurate. It is also incomplete, not because any phase is missing, but because the roadmap describes what to do, not the friction that kills timelines when teams try to do it without FHIR-specific depth.
Most digital health teams underestimate the complexity of FHIR implementation. Not the concept. The actual execution.
Here is what the roadmap does not show.
EHR vendors do not behave like the spec says they should.
Epic’s FHIR R4 implementation exposes roughly 40–60% of the full resource set, and the exposed endpoints vary by organizational configuration. Cerner’s bulk export behavior diverges from the HL7 specification in ways that only surface during sandbox testing, not during architecture.
Teams without prior hands-on experience with these specific quirks spend weeks in discovery that experienced teams skip entirely.
SMART on FHIR authorization is not plug-and-play.
The OAuth 2.0 flows, launch contexts, and scope management behaviors differ meaningfully across EHR platforms. A launch context that works in Epic’s sandbox will not necessarily behave identically in production.
Getting authorization right especially for EHR-embedded app launches requires debugging sessions that inflate Phase 2 and Phase 3 timelines by two to four weeks for teams doing it the first time.
Conformance profiles are where timelines collapse.
Defining implementation guides and mapping your data model to FHIR resources sounds clean on paper. In practice, gaps between your clinical data model and available FHIR resources require decisions with real patient safety implications.
The wrong mapping silently corrupts data without throwing an error. Teams without FHIR architects who have made and documented these decisions before will spend Phase 2 going in circles.
Performance hardening is the phase nobody budgets for correctly.
Running concurrent API calls at realistic patient volumes against a live EHR sandbox is a different problem from running them in development. Response time degradation, rate limiting by the EHR vendor, and authentication token expiry under load are not hypothetical. They show up in every production-scale test and require targeted fixes before Phase 4.
Add these hidden complexity layers to a team’s learning curve, and the industry average for a FHIR implementation from discovery to production sync stretches to 20–24 weeks.
Sometimes longer. The rework in Phases 2 and 3 is where most of it disappears.
How MultiQoS Compresses This to 14 Weeks?
MultiQoS has run FHIR healthcare app development projects from discovery to production sync in under 14 weeks for healthcare clients. That compression is not aggressive scheduling. It is accumulated EHR-specific knowledge applied at every decision point where first-timers slow down.
The difference shows up in four places.
Pre-mapped EHR behavior.
MultiQoS teams have documented Epic and Cerner endpoint behavior, resource availability, and divergence from the HL7 spec across multiple production deployments. Phase 1 discovery does not start from zero. Known quirks are accounted for in the architecture before a single line of code is written.
Tested SMART on FHIR authorization patterns.
Authorization flows for EHR-embedded app launches, standalone app launches, and system-to-system backend connections are pre-validated across the major EHR platforms MultiQoS has deployed against. Phase 2 does not repeat the debugging work that prior projects already absorbed.
Clinical data mapping decisions with precedent.
Where FHIR resources do not cleanly map to a clinical data model, MultiQoS brings documented decisions from prior implementations. The conformance profile work in Phase 2 runs faster because the hard mapping calls have been made before, reviewed, and validated against real EHR data.
Performance baselines from prior production deployments.
Concurrent API call behavior, rate limit thresholds, and token management patterns at scale are known quantities. Phase 3 performance hardening targets the real bottlenecks rather than running exploratory load tests from scratch.
The 10-week gap between a first-time FHIR implementation and a MultiQoS-led one is not a marketing claim. It is the accumulated cost of decisions your team does not have to make from scratch, debugging sessions you do not have to run twice, and rework cycles that do not happen because the architecture was right the first time.
Healthcare app development at this level of compliance and clinical complexity has no margin for a slow learning curve.
Conclusion
The majority of the digital health companies are already operating FHIR APIs, and those that still have proprietary point-to-point interfaces aren’t playing it safe, with ONC calling for the reworking of certification requirements. They’re also building up technical debt, regulatory exposure, and innovation bottlenecks.
With FHIR-based healthcare application development, you can expect faster EHR integration and a 30-50% reduction in integration costs, a built-in HIPAA compliance architecture, and a base for scalable AI pipelines, wearable data, and population health analytics without the need to start over from the ground up.
The future of mobile app development in healthcare runs on FHIR. The organizations that build on that foundation now will not need to play catch-up later.
FAQs
FHIR (Fast Healthcare Interoperability Resources) is a standard of REST APIs, JSON, and OAuth 2.0 that allows real-time exchange of clinical information between any EHR system. FHIR is the integration layer for healthcare application development that allows apps to read, write, and subscribe to clinical information such as patient demographics, observations, conditions, and medications, without requiring a custom interface for each EHR vendor.
The cost of focused FHIR implementation (patient portal or read-only EHR integration) is between $40,000 and $120,000. Other EHR vendors introduce additional costs of configuration, and not full rebuilds. Bidirectional sync with write-back validation costs $50,000 to $80,000 per EHR platform, and can take 10 to 18 weeks, depending on the complexity of clinical workflows.
Read-based FHIR implementations progress through a phased deployment of discovery, architecture, build and test, pilot deployment, and arrive in production in 15-20 weeks. Multi-EHR bidirectional sync takes 20-30 weeks. The time length in Phase 1 will vary according to the scope discipline. Patient demographics groups will always be at the low end of these ranges.
FHIR is not a HIPAA standard, but when implemented correctly, FHIR R4 meets HIPAA requirements. The OAuth 2.0 maps are provided by SMART on FHIR and deal with access control requirements, the AuditEvent resources address audit trail requirements, and TLS 1.2+ is for data-in-transit encryption. The compliance structure is provided by FHIR. Your team supplies the right infrastructure, BAA chain, and access control setup.

Get In Touch
Get Stories in Your Inbox Thrice a Month.


Super Apps: Should Your Enterprise Build an All-in-One Platform
Application Modernization Strategy vs Rebuild vs Replace: How to Pick the Right Path?